Houma: 985.857.8838
Raceland: 985.537.7546
Morgan City: 985.384.9440

Children's ENT
Children's ENT
 Children, by their nature, suffer many illnesses of the ears, nose
and throat. Often, your child’s physician may refer him/her to an otolaryngologist for specialty care. Otolaryngology is the medical specialty that focuses on disorders of the ear, nose, and throat.
Otolaryngologists are also known as ENT physicians.
Children, by their nature, suffer many illnesses of the ears, nose
and throat. Often, your child’s physician may refer him/her to an otolaryngologist for specialty care. Otolaryngology is the medical specialty that focuses on disorders of the ear, nose, and throat.
Otolaryngologists are also known as ENT physicians.
Ear Infections and Earache
What Is Otitis Media?
Otitis media means inflammation of the middle ear. The inflammation occurs as a result of a middle ear infection. It can occur in one or both ears. Otitis media is the most frequent diagnosis recorded for children who visit physicians for illness. It is also the most common cause of hearing loss in children.
Although otitis media is most common in young children, it also affects adults occasionally. It occurs most commonly in the winter and early spring months.
Is It Serious?
Yes, it is serious because of the severe earache and hearing loss it can create. Hearing loss, especially in children, may impair learning capacity and even delay speech development. However, if it is treated promptly and effectively, hearing can almost always be restored to normal.
Otitis media is also serious because the infection can spread to nearby structures in the head, especially the mastoid. Thus, it is very important to recognize the symptoms (see list) of otitis media and to get immediate attention from your doctor.
How Does the Ear Work?
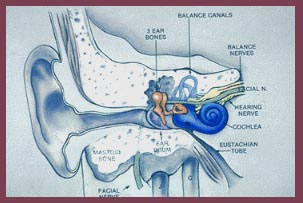 The outer ear collects sounds. The middle ear is a pea sized, air-filled cavity separated from the outer ear by the paper-thin eardrum. Attached to the eardrum are three tiny ear bones. When sound waves strike the eardrum, it vibrates and sets the bones in motion that transmit to the inner ear. The inner ear converts vibrations to electrical signals and sends these signals to the brain. It also helps maintain balance.
The outer ear collects sounds. The middle ear is a pea sized, air-filled cavity separated from the outer ear by the paper-thin eardrum. Attached to the eardrum are three tiny ear bones. When sound waves strike the eardrum, it vibrates and sets the bones in motion that transmit to the inner ear. The inner ear converts vibrations to electrical signals and sends these signals to the brain. It also helps maintain balance.
A healthy middle ear contains air at the same atmospheric pressure as outside of the ear, allowing free vibration. Air enters the middle ear through the narrow eustachian tube that connects the back of the nose to the ear. When you yawn and hear a pop, your eustachian tube has just sent a tiny air bubble to your middle ear to equalize the air pressure.
What Causes Otitis Media?
Blockage of the eustachian tube during a cold, allergy, or upper respiratory infection and the presence of bacteria or viruses lead to the accumulation of fluid (a build-up of pus and mucus) behind the eardrum. This is the infection called acute otitis media. The build up of pressurized pus in the middle ear causes earache, swelling, and redness. Since the eardrum cannot vibrate properly, you or your child may have hearing problems.
Sometimes the eardrum ruptures, and pus drains out of the ear. But more commonly, the pus and mucus remain in the middle ear due to the swollen and inflamed eustachian tube. This is called middle ear effusion or serous otitis media. Often after the acute infection has passed, the effusion remains and becomes chronic, lasting for weeks, months, or even years. This condition makes one subject to frequent recurrences of the acute infection and may cause difficulty in hearing.
What Are the Symptoms?
In infants and toddlers look for pulling or scratching at the ear, especially if accompanied by the following
- hearing problems
- crying, irritability
- fever
- vomiting
- ear drainage
In young children, adolescents, and adults look for:
- earache
- feeling of fullness or pressure
- hearing problems
- dizziness, loss of balance
- nausea, vomiting
- ear drainage
- fever
Remember, without proper treatment, damage from an ear infection can cause chronic or permanent hearing loss.
What Will Happen at the Doctor’s Office?
During an examination, the doctor will use an instrument called an otoscope to assess the ear’s condition. With it, the doctor will perform an examination to check for redness in the ear and/or fluid behind the eardrum. With the gentle use of air pressure, the doctor can also see if the eardrum moves. If the eardrum doesn’t move and/or is red, an ear infection is probably present.
Two other tests may be performed for more information.
- An audiogram tests if hearing loss has occurred by presenting tones at various pitches.
- A tympanogram measures the air pressure in the middle ear to see how well the eustachian tube is working and how well the eardrum can move.
The Importance of Medication
The doctor may prescribe one or more medications. It is important that all the medication(s) be taken as directed and that any follow-up visits be kept. Often, antibiotics to fight the infection will make the earache go away rapidly, but the infection may need more time to clear up. So, be sure that the medication is taken for the full time your doctor has indicated. Other medications that your doctor may prescribe include an antihistamine (for allergies), a decongestant (especially with a cold), or both.
Sometimes the doctor may recommend a medication to reduce fever and/or pain. Analgesic ear drops can ease the pain of an earache. Call your doctor if you have any questions about you or your child’s medication or if symptoms do not clear.
What Other Treatment May Be Necessary?
Most of the time, otitis media clears up with proper medication and home treatment. In many cases, however, further treatment may be recommended by your physician. An operation, called a myringotomy may be recommended. This involves a small surgical incision (opening) into the eardrum to promote drainage of fluid and to relieve pain. The incision heals within a few days with practically no scarring or injury to the eardrum. In fact, the surgical opening can heal so fast that it often closes before the infection and the fluid are gone. A ventilation tube can be placed in the incision, preventing fluid accumulation and thus improving hearing.
The surgeon selects a ventilation tube for your child that will remain in place for as long as required for the middle ear infection to improve and for the eustachian tube to return to normal. This may require several weeks or months. During this time, you must keep water out of the ears because it could start an infection. Otherwise, the tube causes no trouble, and you will probably notice a remarkable improvement in hearing and a decrease in the frequency of ear infections.
Otitis media may recur as a result of chronically infected adenoids and tonsils. If this becomes a problem, your doctor may recommend removal of one or both. This can be done at the same time as ventilation tubes are inserted.
Allergies may also require treatment.
 So, Remember . . .
So, Remember . . .
Otitis media is generally not serious if it is promptly and properly treated. With the help of your physician, you and/or your child can feel and hear better very soon.
Be sure to follow the treatment plan, and see your physician until he/she tells you that the condition is fully cured.
Doctor, Please Explain Ear Tubes
Painful ear infections are a rite of passage for children – by the age of five, nearly every child has experienced at least one episode. Most ear infections either resolve on their own (viral) or are effectively treated by antibiotics (bacterial). But sometimes, ear infections and/or fluid in the middle ear may become a chronic problem leading to other issues such as hearing loss, behavior, and speech problems. In these cases, insertion of an ear tube by an otolaryngologist (ear, nose, and throat surgeon) may be considered.
What are ear tubes?
Ear tubes are tiny cylinders placed through the ear drum (tympanic membrane) to allow air into the middle ear. They also may be called tympanostomy tubes, myringotomy tubes, ventilation tubes, or PE (pressure equalization) tubes. These tubes can be made out of plastic, metal, or Teflon and may have a coating intended to reduce the possibility of infection. There are two basic types of ear tubes: short-term and long-term. Short-term tubes are smaller and typically stay in place for six months to a year before falling out on their own. Long-term tubes are larger and have flanges that secure them in place for a longer period of time. Long term tubes may fall out on their own, but removal by an otolaryngologist is often necessary.
Who needs ear tubes and why?
Ear tubes are often recommended when a person experiences repeated middle ear infection (acute otitis media) or has hearing loss caused by the persistent presence of middle ear fluid (otitis media with effusion). These conditions most commonly occur in children, but can also be present in teens and adults and can lead to speech and balance problems, hearing loss, or changes in the structure of the ear drum. Other less common conditions that may warrant the placement of ear tubes are malformation of the ear drum or Eustachian tube, Down Syndrome, cleft palate, and barotrauma (injury to the middle ear caused by a reduction of air pressure), usually seen with altitude changes such as flying and scuba diving.
Each year, more than half a million ear tube surgeries are performed on children, making it the most common childhood surgery performed with anesthesia. The average age of ear tube insertion is one to three years old. Inserting ear tubes may:
- reduce the risk of future ear infection,
- restore hearing loss caused by middle ear fluid,
- improve speech problems and balance problems, and
- improve behavior and sleep problems caused by chronic ear infections.
How are ear tubes inserted in the ear?
Ear tubes are inserted through an outpatient surgical procedure called a myringotomy. A myringotomy refers to an incision (a hole) in the ear drum or tympanic membrane. This is most often done under a surgical microscope with a small scalpel (tiny knife), but it can also be accomplished with a laser. If an ear tube is not inserted, the hole would heal and close within a few days. To prevent this, an ear tube is placed in the hole to keep it open and allow air to reach the middle ear space (ventilation).
What happens during surgery?
A light general anesthetic (laughing gas) is administered for young children. Some older children and adults may be able to tolerate the procedure without anesthetic. A myringotomy is performed and the fluid behind the ear drum (in the middle ear space) is suctioned out. The ear tube is then placed in the hole. Ear drops may be administered after the ear tube is placed and may be necessary for a few days. The procedure usually lasts less than 15 minutes and patients awaken quickly. Sometimes the otolaryngologist will recommend removal of the adenoid tissue (lymph tissue located in the upper airway behind the nose) when ear tubes are placed. This is often considered when a repeat tube insertion is necessary. Current research indicates that removing adenoid tissue concurrent with placement of ear tubes can reduce the risk of recurrent ear infection and the need for repeat surgery.
What to expect after surgery?
After surgery, the patient is monitored in the recovery room and will usually go home within an hour if no complications are present. Patients usually experience little or no postoperative pain but grogginess, irritability, and/or nausea from the anesthesia can occur temporarily. Hearing loss caused by the presence of middle ear fluid is immediately resolved by surgery. Sometimes children can hear so much better that they complain that normal sounds seem too loud. The otolaryngologist will provide specific postoperative instructions for each patient including when to seek immediate attention and follow-up appointments. He or she may also prescribe antibiotic ear drops for a few days.
To avoid the possibility of bacteria entering the middle ear through the ventilation tube, physicians may recommend keeping ears dry by using ear plugs or other water-tight devices during bathing, swimming, and water activities. However, recent research suggests that protecting the ear may not be necessary, except when diving or engaging in water activities in unclean water such as lakes and rivers. Parents should consult with the treating physician about ear protection after surgery.
Possible complications
Myringotomy with insertion of ear tubes is an extremely common and safe procedure with minimal complications. When complications do occur, they may include:
- Perforation – This can happen when a tube comes out or a long-term tube is removed and the hole in the tympanic membrane (ear drum) does not close. The hole can be patched through a minor surgical procedure called a tympanoplasty or myringoplasty.
- Scarring – Any irritation of the ear drum (recurrent ear infections), including repeated in-sertion of ear tubes, can cause scarring called tympanosclerosis or myringosclerosis. In most cases, this causes no problems with hearing.
- Infection – Ear infections can still occur in the middle ear or around the ear tube. However, these infections are usually less frequent, result in less hearing loss, and are easier to treat – often only with ear drops. Sometimes an oral antibiotic is still needed.
- Ear tubes come out too early or stay in too long – If an ear tube expels from the ear drum too soon (which is unpredictable), fluid may return and repeat surgery may be needed. Ear tubes that remain too long may result in perforation or may require removal by the otolaryngologist.
Doctor, Explain Tonsils and Adenoids
Insight into Tonsillectomy and Adenoidectomy
Tonsils and adenoids are masses of tissue that are similar to the lymph nodes or "glands" found in the neck, groin, and armpits. Tonsils are the two masses on the back of the throat. Adenoids are high in the throat behind the nose and the roof of the mouth (soft palate) and are not visible through the mouth without special instruments.
Tonsils and adenoids are near the entrance to the breathing passages where they can catch incoming germs, which cause infections. They "sample" bacteria and viruses and can become infected themselves. Scientists believe they work as part of the body's immune system by filtering germs that attempt to invade the body, and that they help to develop antibodies to germs.
This happens primarily during the first few years of life, becoming less important as we get older. Children who must have their tonsils and adenoids removed suffer no loss in their resistance.
What Affects Tonsils and Adenoids?
The most common problems affecting the tonsils and adenoids are recurrent infections (throat or ear) and significant enlargement or obstruction that causes breathing and swallowing problems.
Abscesses around the tonsils, chronic tonsillitis, and infections of small pockets within the tonsils that produce foul-smelling, cheese-like formations can also affect the tonsils and adenoids, making them sore and swollen. Tumors are rare, but can grow on the tonsils.
When Should I See My Doctor?
You should see your doctor when you or your child suffer the common symptoms of infected or enlarged tonsils or adenoids.
The Exam
The primary methods used to check tonsils and adenoids are:
- Medical history
- Physical examination
- Throat cultures/Strep tests
- X-rays
- Blood tests
What Should I Expect At the Exam?
Your physician will ask about problems of the ear, nose, and throat and examine the head and neck. He or she will use a small mirror or a flexible lighted instrument to see these areas.
Cultures/strep tests are important in diagnosing certain infections in the throat, especially "strep" throat.
X-rays are sometimes helpful in determining the size and shape of the adenoids. Blood tests can determine problems such as mononucleosis.
How Are Tonsil and Adenoid Diseases Treated?
Bacterial infections of the tonsils, especially those caused by streptococcus, are first treated with antibiotics. Sometimes, removal of the tonsils and/or adenoids may be recommended. The two primary reasons for tonsil and/or adenoid removal are (1) recurrent infection despite antibiotic therapy and (2) difficulty breathing due to enlarged tonsils and/or adenoids.
Such obstruction to breathing causes snoring and disturbed sleep that leads to daytime sleepiness in adults and behavioral problems in children. Some orthodontists believe chronic mouth breathing from large tonsils and adenoids causes malformations of the face and improper alignment of the teeth.
Chronic infection can affect other areas such as the eustachian tube – the passage between the back of the nose and the inside of the ear. This can lead to frequent ear infections and potential hearing loss.
Recent studies indicate adenoidectomy may be a beneficial treatment for some children with chronic earaches accompanied by fluid in the middle ear (otitis media with effusion).
In adults, the possibility of cancer or a tumor may be another reason for removing the tonsils and adenoids.
In some patients, especially those with infectious mononucleosis, severe enlargement may obstruct the airway. For those patients, treatment with steroids (e.g., cortisone) is sometimes helpful.
Tonsillitis and Its Symptoms
Tonsillitis is an infection in one or both tonsils. One sign is swelling of the tonsils. Other signs or symptoms are:
• Redder than normal tonsils
• A white or yellow coating on the tonsils
• A slight voice change due to swelling
• Sore throat
• Uncomfortable or painful swallowing
• Swollen lymph nodes (glands) in the neck
• Fever
• Bad breath
Enlarged Adenoids and Their Symptoms
If you or your child's adenoids are enlarged, it may be hard to breathe through the nose.
Other signs of constant enlargement are:
• Breathing through the mouth instead of the nose most of the time
• Nose sounds "blocked" when the person speaks
• Noisy breathing during the day
• Recurrent ear infections
• Snoring at night
• Breathing stops for a few seconds at night during snoring or loud breathing (sleep apnea)
Surgery
Your child: Talk to your child about his/her feelings and provide strong reassurance and support throughout the process. Encourage the idea that the procedure will make him/her healthier. Be with your child as much as possible before and after the surgery. Tell him/her to expect a sore throat after surgery. Reassure your child that the operation does not remove any important parts of the body, and that he/she will not look any different afterward. If your child has a friend who has had this surgery, it may be helpful to talk about it with that friend.
Adults and children: For at least two weeks before any surgery, the patient should refrain from taking aspirin or other medications containing aspirin. (WARNING: Children should never be given aspirin because of the risk of developing Reye's syndrome).
- If the patient or patient's family has had any problems with anesthesia, the surgeon should be informed. If the patient is taking any other medications, has sickle cell anemia, has a bleeding disorder, is pregnant, has concerns about the transfusion of blood, or has used steroids in the past year, the surgeon should be informed.
- A blood test and possibly a urine test may be required prior to surgery.
- Generally, after midnight prior to the operation, nothing (chewing gum, mouthwashes, throat lozenges, toothpaste, water) may be taken by mouth. Anything in the stomach may be vomited when anesthesia is induced, and this is dangerous.
When the patient arrives at the hospital or surgery center, the anesthesiologist or nursing staff may meet with the patient and family to review the patient's history. The patient will then be taken to the operating room and given an anesthetic. Intravenous fluids are usually given during and after surgery.
After the operation, the patient will be taken to the recovery area. Recovery room staff will observe the patient until discharged. Every patient is special, and recovery times vary for each individual. Many patients are released after 2–10 hours. Others are kept overnight. Intensive care may be needed for select cases.
Your ENT specialist will provide you with the details of pre-operative and postoperative care and answer any questions you may have.
After Surgery
There are several postoperative symptoms that may arise. These include (but are not limited to) swallowing problems, vomiting, fever, throat pain, and ear pain. Occasionally, bleeding may occur after surgery. If the patient has any bleeding, your surgeon should be notified immediately.
Allergic Rhinitis (Hay Fever)
Allergic rhinitis (hay fever) is an especially common chronic nasal problem in adolescents and young adults. Allergies to inhalants like pollen, dust, and animal dander begin to cause sinus and nasal symptoms in early childhood. Infants and young children are especially susceptible to allergic sensitivity to foods and indoor allergens.
What causes allergic rhinitis?
Allergic rhinitis typically results from two conditions: family history/genetic predisposition to allergic disease and exposure to allergens. Allergens are substances that produce an allergic response.
Children are not born with allergies but develop symptoms upon repeated exposure to environmental allergens. The earliest exposure is through food—and infants may develop eczema, nasal congestion, nasal discharge, and wheezing caused by one or more allergens (milk protein is the most common). Allergies can also contribute to repeated ear infections in children. In early childhood, indoor exposure to dust mites, animal dander, and mold spores may cause an allergic reaction, often lasting throughout the year. Outdoor allergens including pollen from trees, grasses, and weeds primarily cause seasonal symptoms.
The number of patients with allergic rhinitis has increased in the past decade, especially in urban areas. Before adolescence, twice as many boys as girls are affected; however, after adolescence, females are slightly more affected than males. Researchers have found that children born to a large family with several older siblings and day care attendance seem to have less likelihood of developing allergic disease later in life.
What are allergic rhinitis symptoms?
Symptoms can vary with the season and type of allergen and include sneezing, runny nose, nasal congestion, and itchy eyes and nose. A year-long exposure usually produces nasal congestion (chronic stuffy nose).
In children, allergen exposure and subsequent inflammation in the upper respiratory system cause nasal obstruction. This obstruction becomes worse with the gradual enlargement of the adenoid tissue and the tonsils inherent with age. Consequently, the young patient may have mouth-breathing, snoring, and sleep-disordered breathing such as obstructive sleep apnea. Sleep problems such as insomnia, bed-wetting, and sleepwalking may accompany these symptoms along with behavioral changes including short attention span, irritability, poor school performance, and excessive daytime sleepiness.
In these patients, upper respiratory infections such as colds and ear infections are more frequent and last longer. A child’s symptoms after exposure to pollutants such as tobacco smoke are usually amplified in the presence of ongoing allergic inflammation.
When should my child see a doctor?
If your child’s cold-like symptoms (sneezing and runny nose) persist for more than two weeks, it is appropriate to contact a physician.
Emergency treatment is rarely necessary except for upper airway obstruction causing severe sleep apnea or an anaphylactic reaction caused by exposure to a food allergen. Treatment of anaphylactic shock should be immediate and requires continued observation and care.
What happens during a physician visit?
The doctor will first obtain an extensive history about the child, the home environment, possible exposures, and progression of symptoms. Family history of atopic/allergic disease and the presence of other disorders such as eczema and asthma strongly support the diagnosis of allergic rhinitis. The physician will seek a link between the symptoms and exposure to certain allergens.
he physician will examine the skin, eyes, face and facial structures, ears, nose, and throat. In some cases, a nasal endoscopy may be performed. If the history and the physical exam suggest allergic rhinitis, a screening allergy test is ordered. This can be a blood test or a skin prick test. In most children it is easier to obtain a blood test known as the RadioAllergoSorbent Test or RAST. This test measures the amount of specific Immunoglobulin E antibodies (IgE) in the blood responding to various environmental and food allergens.
The skin test results, often immediately available, may be affected by the recent use of antihistamines and other medications, dermatologic conditions, and age of the patient. The blood test is not affected by medication, and results are usually available in several days.
How is allergic rhinitis treated?
The most common treatment recommendation is to have the child avoid the allergens causing the allergic sensitivity. The physician will work with caregivers to develop an avoidance strategy based on the nature of the allergen, exposure, and availability of avoidance measures.
Cost and lifestyle are important factors to consider. For mild, seasonal allergies, avoidance could be the most effective course of action. If pet dander is the offender, consideration should be given to removing the pet from the child’s environment.
Severe symptoms, multiple allergens, year-long exposure, and limited resources for environmental control may call for additional treatment measures. Nasal saline irrigations, nasal steroid sprays, and non-sedating antihistamines are indicated for symptom control. Nasal steroids are the most effective in reducing nasal symptoms of allergic rhinitis. A short burst of oral steroids may be appropriate for some patients with severe symptoms or to gain control during acute attacks.
If symptoms are severe and due to multiple allergens, the child is symptomatic more than six months in a year, and if all other measures fail, then immunotherapy (IT) (or desensitization) may be suggested. IT is delivered by injections of the allergen in doses that are increased incrementally to a maximum that is tolerated without a reaction. Maintenance injections can be delivered at increasing intervals starting from weekly to bi-weekly to monthly injections for up to three to five years. Children with pollen sensitivities benefit most from this treatment. IT is also effective in reducing the onset of pollen-induced asthma.
Pediatric Sinusitis
Your child’s sinuses are not fully developed until age 20. Although small, the maxillary (behind the cheek) and ethmoid (between the eyes) sinuses are present at birth. Unlike in adults, pediatric sinusitis is difficult to diagnose because symptoms can be subtle and the causes complex.
How do I know when my child has sinusitis?
The following symptoms may indicate a sinus infection in your child:
• a “cold” lasting more than 10 to 14 days, sometimes with a low-grade fever thick,
• yellow-green nasal drainage
• post-nasal drip, sometimes leading to or exhibited as sore throat, cough, bad breath, nausea, and/or vomiting
• headache, usually in children age six or older
• irritability or fatigue
• swelling around the eyes
Young children have immature immune systems and are more prone to infections of the nose, sinus, and ears, especially in the first several years of life. These are most frequently caused by viral infections (colds), and they may be aggravated by allergies. However, when your child remains ill beyond the usual week to ten days, a serious sinus infection is likely.
You can reduce the risk of sinus infections for your child by reducing exposure to known allergens and pollutants such as tobacco smoke, reducing his/her time at day care, and treating stomach acid reflux disease.
How will the doctor treat sinusitis?
- Acute sinusitis: Most children respond very well to antibiotic therapy. Nasal decongestants or topical nasal sprays may also be prescribed for short-term relief of stuffiness. Nasal saline (saltwater) drops or gentle spray can be helpful in thinning secretions and improving mucous membrane function. If your child has acute sinusitis, symptoms should improve within the first few days. Even if your child improves dramatically within the first week of treatment, it is important that you continue therapy until all the antibiotics have been taken. Your doctor may decide to treat your child with additional medicines if he/she has allergies or other conditions that make the sinus infection worse.
- Chronic sinusitis: If your child suffers from one or more symptoms of sinusitis for at least 12 weeks, he or she may have chronic sinusitis. Chronic sinusitis or recurrent episodes of acute sinusitis numbering more than four to six per year are indications that you should seek consultation with an ear, nose, and throat (ENT) specialist. The ENT may recommend medical or surgical treatment of the sinuses.
- Diagnosis of sinusitis: If your child sees an ENT specialist, the doctor will examine his/her ears, nose, and throat. A thorough history and examination usually leads to the correct diagnosis. Occasionally, special instruments will be used to look into the nose during the office visit. An x-ray called a CT scan may help to determine how your child's sinuses are formed, where the blockage has occurred, and the reliability of a sinusitis diagnosis.
When is surgery necessary?
Only a small percentage of children with severe or persistent sinusitis require surgery to relieve symptoms that do not respond to medical therapy. Using an instrument called an endoscope, the ENT surgeon opens the natural drainage pathways of your child's sinuses and makes the narrow passages wider. This also allows for culturing so that antibiotics can be directed specifically against your child's sinus infection. Opening up the sinuses and allowing air to circulate usually results in a reduction in the number and severity of sinus infections.
Your doctor may advise removing adenoid tissue from behind the nose as part of the treatment for sinusitis. Although the adenoid tissue does not directly block the sinuses, infection of the adenoid tissue, called adenoiditis, or obstruction of the back of the nose, can cause many of the symptoms that are similar to sinusitis, namely, runny nose, stuffy nose, post-nasal drip, bad breath, cough, and headache.
Sinusitis in children is different than sinusitis in adults. Children more often demonstrate a cough, bad breath, crankiness, low energy, and swelling around the eyes along with a thick yellow-green nasal or post-nasal drip. Once the diagnosis of sinusitis has been made, children are successfully treated with antibiotic therapy in most cases. If medical therapy fails, surgical therapy can be used as a safe and effective method of treating sinus disease in children.